Dr. Manasi Thakur | Gynaecologist In Nagpur | Pregnancy, Delivery | Abortion | Cosmetic Gynecology
Cesarean Section | Dr. Manasi Thakur – Zenith Hospital, Nagpur
Why is a C-section Done?
In some cases, a cesarean section is safer than a vaginal delivery. Common reasons include:
Labour not progressing – when there is no further dilation of the cervix or descent of the baby’s head.
Fetal distress – persistent signs of distress on CTG.
Abnormal position of the baby – e.g., breech (feet/buttocks first) or transverse (shoulder first).
Multiple pregnancies – especially when twins/triplets are not in safe positions.
Abnormal placentation – placenta previa, placenta accreta/increta/percreta.
Cord prolapse – when the umbilical cord slips into the vagina, causing acute fetal distress.
Maternal illness – such as severe heart disease, uncontrolled blood pressure, or active genital herpes.
Cephalo-pelvic disproportion (CPD) – baby’s head is too large or pelvis is too small.
Previous C-sections – depending on recovery, number of scars, and delivery conditions. VBAC may be possible in some women, but repeat C-section is often safer after multiple surgeries.
Risks of C-section
For the Baby:
Breathing problems (especially transient tachypnea in the first few days).
Rare accidental surgical injury.
For the Mother:
Postpartum hemorrhage (heavy bleeding).
Infections (uterine lining or incision site).
Anesthesia risks (allergic or adverse reactions).
Surgical injury (rare but possible to bladder or bowel).
Blood clots (higher in women with obesity, smoking, or prolonged bed rest).
Future pregnancies – higher risk of placenta previa, accreta, or uterine rupture.
Preparation for C-section
Planned surgery – date fixed in advance, blood tests, and anesthetist consultation.
Discussion – ask questions, clarify doubts, and discuss permanent birth control if desired.
Before hospital admission – antiseptic shower, fasting 6–8 hours
What to Expect
Before the Procedure
At hospital: IV line for fluids/medications, antibiotics, abdominal prep, catheter placement.
Anesthesia – usually spinal (numbs lower body), sometimes general in emergencies.
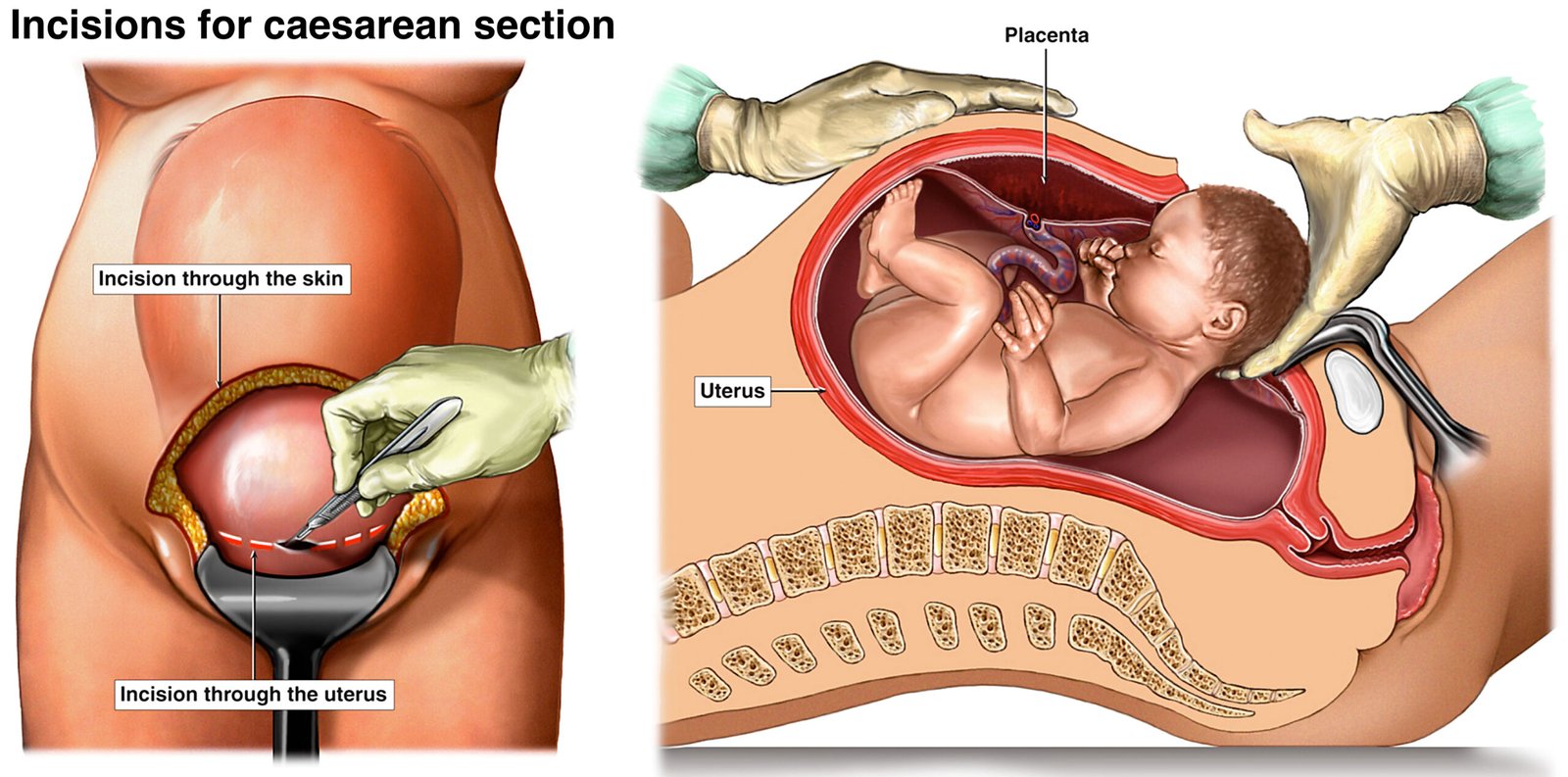
During the Procedure
Abdominal incision – usually a low-transverse (Pfannenstiel) cut; sometimes vertical if required.
Uterine incision – horizontal cut on the lower uterus.
Delivery of baby – head first (cephalic), or buttocks/shoulders if breech/transverse.
Placenta removal and closure – uterus and abdomen stitched layer by layer.
After the Procedure
Hospital stay: usually 3 days.
Breastfeeding encouraged early.
Fluids and diet resumed gradually after 6–8 hours.
Catheter removed after ~24 hours.
Regular antibiotics, painkillers, and IV fluids given.
Baby’s vaccinations ensured before discharge.
Recovery at Home
Take prescribed medicines (antibiotics, painkillers, probiotics).
Rest and breastfeed frequently (every 2 hours).
Avoid heavy lifting and straining.
No sex for 6 weeks to prevent infection.
Avoid driving until at least 2 weeks, or until you can brake comfortably.
Report immediately if you notice:
Redness, swelling, or discharge from incision
Fever
Heavy bleeding
Severe pain
Depression, mood swings, or loss of appetite
Follow-Up Care
Post-partum recovery is ongoing. Visits are recommended:
Within 3 weeks of delivery
Again by 12 weeks postpartum
At Zenith Hospital, Nagpur, Dr. Manasi Thakur provides complete post-partum care, including physical and emotional well-being, guidance on family planning, and support for new mothers.